

Congenital Anomalies in Riyadh are defined by a diverse and complex epidemiological landscape, representing a significant portion of pediatric healthcare delivery within the city’s tertiary care institutions. The structural birth defect spectrum in the region is shaped by a confluence of genetic predisposition, maternal health variables, and the evolving sophistication of prenatal and neonatal diagnostics. By analyzing the structural patterns across this population, healthcare professionals can better tailor preventive strategies and surgical interventions to address the unique needs of the pediatric demographic.
Understanding the Structural Spectrum
The structural birth defect spectrum in Riyadh spans a broad range of developmental abnormalities, from isolated defects to those associated with complex syndromes. Unlike some populations where environmental factors might dominate the epidemiological profile, the data in Riyadh consistently highlights a high prevalence of conditions with a strong hereditary component. This is particularly evident in the frequency of musculoskeletal, cardiovascular, and urogenital anomalies, which frequently appear as the primary diagnostic categories in clinical records.
The classification of these defects is essential for clinical management. Researchers and practitioners generally categorize these into:
-
Cardiovascular Anomalies: As the most frequent category, these involve structural defects of the heart and great vessels, requiring rigorous assessment and often, timely surgical intervention.
-
Musculoskeletal Malformations: This category includes a variety of limb deficiencies, congenital hip dysplasia, and spinal abnormalities, often requiring long-term orthopedic management.
-
Craniofacial Anomalies: Conditions such as cleft lip and palate are prevalent and necessitate a multidisciplinary team approach involving plastic surgeons, speech therapists, and orthodontists.
-
Urogenital and Gastrointestinal Anomalies: These structural defects often present with functional implications that require specialized pediatric surgical care and early postnatal monitoring.
The Impact of Consanguinity and Genetic Factors
A defining feature of the epidemiological spectrum in Riyadh is the substantial influence of consanguinity. Numerous studies conducted within the city’s academic and medical centers have demonstrated that the elevated rate of marriage between close relatives is a primary driver for the increased incidence of recessive structural disorders. When assessing the pediatric population, clinical geneticists often find that the spectrum of defects is heavily skewed toward autosomal recessive patterns, which poses unique challenges for family planning and prenatal counseling.
The genetic architecture of the population is not merely a statistical figure but a daily clinical reality. The high prevalence of these structural defects necessitates an infrastructure that integrates genetic testing—such as chromosomal microarrays—into the standard diagnostic workup for infants presenting with multiple malformations. This genetic-focused approach has enabled a more precise understanding of the etiology behind the structural spectrum, moving away from generalized assessments toward targeted diagnostic medicine.
Maternal Health and Environmental Interventions
Beyond genetics, the epidemiological spectrum is influenced by maternal health. The prevalence of gestational diabetes and maternal obesity has been identified as a significant risk factor for a wide range of structural anomalies, particularly those affecting the cardiovascular and central nervous systems. Clinical observations in Riyadh underscore that optimizing maternal health during the periconceptional period—particularly through the management of chronic conditions and nutritional supplementation—is one of the most effective ways to mitigate the risk of these defects.
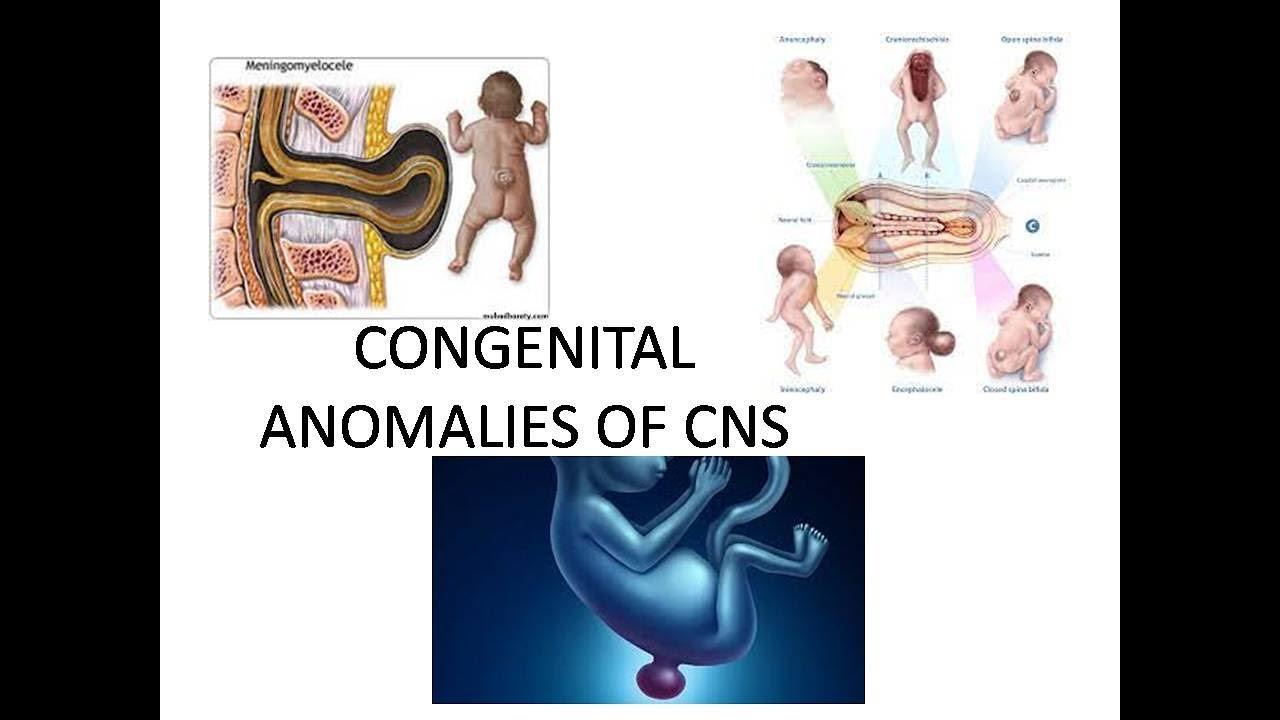
Public health initiatives have focused heavily on the necessity of folic acid supplementation, which is critical in preventing neural tube defects. The success of these programs in the local pediatric population serves as a template for how broad interventions can influence the structural spectrum of birth defects over time. As these preventive efforts become more ingrained in the healthcare system, there is an expectation that the overall burden of preventable structural abnormalities will continue to decline.
Clinical Strategy and Future Outlook
The future of managing structural birth defects in Riyadh lies in the advancement of "precision pediatrics." This involves moving beyond reactive treatment toward a model of early identification and personalized management. The growth of specialized fetal medicine units within tertiary care centers has been a major milestone, allowing for the prenatal identification of structural defects that were previously only diagnosed at birth. This early window of opportunity allows for surgical planning and parental support, which fundamentally improves the long-term prognosis for the affected child.
As the epidemiological spectrum continues to be mapped with greater granularity, the medical community is moving toward a more collaborative, data-sharing environment. The goal is to build a comprehensive, city-wide registry that tracks these anomalies from prenatal screening through to long-term pediatric follow-up. By doing so, clinicians can not only improve individual patient care but also gain the necessary insights to reduce the overall prevalence of structural birth defects, ensuring a healthier future for the pediatric population in Riyadh.